
The WHO regime - what does it all mean?
The WHO regime - what does it all mean?
A reader’s guide to the International Health Regulations and the pandemic treaty

In order to understand ‘what just happened’ at the 77th World Health Assembly in Geneva last week, we need to understand not just what changed in the International Health Regulations (IHR), but how it all fits together.
In this article I outline the whole scheme based on the amended IHR, and also how the proposed pandemic treaty fits in.
My personal take? I am not feeling relieved that some of the provisions which had been on the negotiating table didn’t end up in the final version. The fundamentals of the scheme are in place, including a new financial mechanism; and negotiations will continue on the treaty. The threat of our governments taking direction from the WHO about what we should do locally about a public health issue is as strong as ever. It happened during the COVID years, and governments around the world seem keen to do it again: if the WHO says so, we’ll do it, whatever that may be. We will commit to doing it. Why? We will not find a coherent rationale based on health, because it’s not about health, it’s a global health products business, and countries appear to be negotiating to protect their financial interests. At least that’s the only way I can make sense of it. When the world believes it needs massive amounts of health products, the only thing that seems to matter is: can we get hold of enough? And can we maximise our share in the profits if we’ve provided the genetic samples from which the health products are produced?
Summary
The whole WHO regime and what to do about it - key messages for your politician:
The WHO is all about money and power; it’s not about health.
It may be in the national interest financially to participate in the WHO regime, but it’s certainly not in our health interests. Australians must be able to make our own public health decisions without being obliged to follow the WHO’s recommended health measures.
Individuals must be able to make their own health decisions. Emergency laws and other regulatory arrangements in each country which enable the enforcement of blanket clinical “guidelines”, and the censoring of doctors who don’t toe the WHO line, must be dismantled.
Billions of dollars can be better spent in other ways, to improve health outcomes.
We are realising that there’s something wrong with how our governments behaved during COVID, and the more we understand about the WHO, the more we are outraged. Politicians will find that they must oppose the WHO if they want to get re-elected.
The WHO isn’t what we thought it was. We do not need the WHO to keep us safe. We need to exit the WHO in order to be safe. We need to disband it.
The basic premise
The basic premise behind the whole scheme is:
more pandemics are inevitable
pandemics pose a serious threat
the serious threat warrants a centralised global response
the solution is pharmaceuticals.
All of these are contestable, and this is what we should be debating. See here for example. Instead, we find our country representatives focusing on one thing and one thing only - health products to “keep us safe” during emergencies.
The never-ending cycle of health emergencies
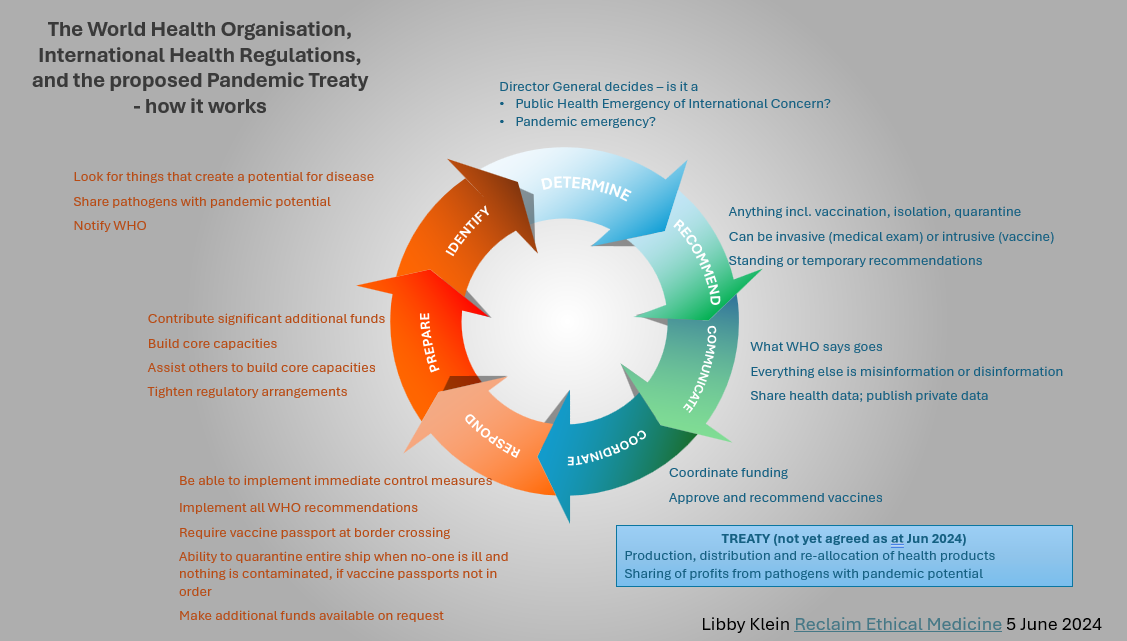
The WHO regime is “always on” and involves a 7-part cycle: Prepare, Identify, Determine, Recommend, Coordinate, Communicate, and Respond.
To understand the scheme which is in place, I recommend reading the International Health Regulations in 2 stages:
1. Read it from beginning to end, highlight a few things that jump out, but don’t worry about trying to understand it completely first time around (the cross references will drive you crazy)
2. Read it again, this time by topic as outlined below – I hope this helps you get your head around it. The relevant articles of the IHR are listed under each heading and my comments are in italics. You might even want to play IHR bingo - see if you can find the relevant article for each bullet point below.
Don’t be put off by the weird numbering - eg “Article 44bis” is called that because they had to squeeze it in between 44 and 45, and didn’t want to renumber the whole document.
Prepare
Articles 2, 4, 5(1), 13(1), 19(a), 35, 44, 44bis, 54bis, Annex 1.
Countries must:
beef up their regulatory arrangements to ensure they can enforce compliance with WHO directives themselves locally – your government does it to you, not the WHO
assist other countries to do the same, with logistics, technical expertise and very significant funding (more than $30bn USD pa)
implement digital health documents (vaccine passports)
collaborate
What’s new?
the concept of preparing
each country must have a “National IHR Authority” as well as a “Focal Point”
financing provisions - a new Coordinating Financial Mechanism (see further below under “Respond”)
a new Committee to oversee implementation (“States Parties Committee for the Implementation of the International Health Regulations (2005)”)
Identify
Article 5, Annex 1
Countries must invest time and money to ensure they have the “core capacities” to detect, assess, notify and report “events”. (They use the term “surveillance”. ) An event is “a manifestation of disease or an occurrence that creates a potential for disease”.
What’s new?
Not much is new on this front in the IHR, but the proposed pandemic treaty has a heavy emphasis on surveillance for disease, “pathogens with pandemic potential”, and anything else under the sun that could conceivably represent a health risk, and which could therefore serve as a trigger for declaring an emergency and implementing controls over who has to take what health products.
Determine
Articles 1 (definitions of public health emergency of international concern and pandemic emergency), 12, 49, Annex 2
The Director General of the WHO has the sole discretion to declare the beginning and end of a Public Health Emergency of International Concern and to determine whether it is also a ‘pandemic emergency’, and is accountable to no-one in doing so:
there are no objective criteria for what constitutes a Public Health Emergency of International Concern, just a series of considerations
an Emergency Committee, whose members are appointed by the Director General, provides its views to the Director General; the Director General then makes a final determination.
What’s new?
The concept of “pandemic emergency”
Anything the Director General feels is a risk can be the basis for the declaration of a public health emergency of international concern, and the issuing of recommendations. This includes climate change, which is specifically mentioned in the preamble to the proposed pandemic treaty. So, we don’t have to have a pandemic for the WHO to assume authority to declare a public health emergency – just circumstances they choose to regard as representing a risk to public health. In the preamble to the pandemic treaty, the need for “resolute action” on “the social environmental, cultural, political and economic determinants of health” is stressed, in order to “combat health emergencies and achieve greater health equity”, indicating that any concern about anything can be packaged as a risk to public health which can then trigger emergency arrangements dictated by the WHO.
Recommend
Articles 13, 15, 16, 17, 18, 24, 40, 43, 47, 48, 49, 50, 53, Annex 6
The Director General can issue any recommendation he or she likes. The list is not a finite one, and it’s not new. The Director General does not have to take the advice of the expert committee, but does have to consider the availability and affordability of a health product before recommending it.
The Director General can issue recommendations whenever he or she wants to:
temporary recommendations where there is a pandemic emergency OR any other type of public health emergency of international concern;
standing recommendations at other times.
Medical treatments including vaccination can be forced if local law allows.
Only products approved by the WHO will be valid for travel. **NEW**
Sick people and contaminated goods can be isolated.
Suspect people and goods can be quarantined.
Ships/planes/trains/border control must be required by local law to comply with recommendations for people in transit, whether on board, embarking or disembarking **NEW**
Countries can have their own additional health measures; these can be invasive (eg medical exam) or intrusive (eg vaccine) subject to WHO’s guidance.
What’s new?
Drug regulation is centralised in the hands of the WHO, giving the WHO an effective monopoly:
Local drug regulators (FDA, TGA etc) can do their own regulatory approvals - but only products approved by the WHO will be good for travel.
The WHO will provide its dossier of information on a health product, which it gets from the manufacturer, to regulators so that they can rubber stamp the product with local approval.
The Director General has to provide supporting evidence to countries when making recommendations.
Requirement for local law enforcement to ensure all forms of transport impose the WHO’s recommendations on passengers at all times, whether they are on board, embarking or disembarking (Why was it important to add this in??)
Many more references to quarantine (the term used when there is no sign of actual illness, only a suspicion). If I don’t have an up-to-date vaccine passport, does that mean I could be deemed to be a suspect person??
Even if there’s no pandemic happening, you can only travel if you’ve had a WHO-approved vaccine. (It’s a racket – WHO gets most of its funding directly or indirectly from BigPharma). For individuals, this means if you want to travel, regardless of whether there is a pandemic at the time, you risk being vaccinated on arrival. There are only limited categories of exemptions, defined by WHO. Past infection is not one of them – proposed new article 36(3) which would have allowed for this did not make it to the final version.
Communicate
Articles 11, 45, 49(6), 53(f), Annex 1
The WHO:
disseminates information about public health events.
can disclose individual personal health data.
is the arbiter of truth - it decides what is “information” and what is “misinformation” or “disinformation”.
issues recommendations.
issues clinical guidance.
has a direct line of communication with health officials.
What’s new?
the requirement to “address” misinformation and disinformation. The language in previous drafts was “counter” but “address” sounds nicer. The terms “misinformation” and “disinformation” are not defined.
the WHO having formal (ostensible) authority to issue clinical guidance for enforcement around the world, inhibiting your doctor from treating you in any other way regardless of your preferences, and regardless of what your doctor thinks is best for you given your personal health situation.
Coordinate
Articles 1, 13, 14, 15, 16
The WHO:
coordinates production, distribution and allocation of health products globally.
What’s new?
the WHO being the global coordinator of production, allocation, and distribution of “relevant health products” which are “those health products needed to respond to public health emergencies of international concern, including pandemic emergencies, which may include medicines, vaccines, diagnostics, medical devices, vector control products, personal protective equipment, decontamination products, assistive products, antidotes, cell- and gene-based therapies, and other health technologies”. Note that health products can be recommended for any type of public health emergency of international concern, not just pandemics.
The proposed pandemic treaty will also have a lot to say about how the production, distribution and allocation of health products will work (see further below).
Respond
Articles 4, 13, 15, 16, 44, 44bis, Annex 1(4)
Countries:
are obliged to follow health measures.
must be able to “implement immediately preliminary control measures”.
will be expected or even required (time will tell) to provide significant funding under the new Coordinating Financial Mechanism, both on an ongoing basis and in response to specific emergencies. The Coordinating Financial Mechanism is to be overseen by the World Health Assembly. (Give us billions and we’ll make sure we use it wisely.)
It makes no difference that recommendations are expressed to be “non-binding”. Countries are obliged to implement health measures recommended under the IHR.
And finally some details about the treaty, which is still being negotiated:
The proposed pandemic treaty – key themes and items of interest
Focus is on health products and how to share the financial and non-financial benefits from production of health products on a massive scale (eg Treaty Art 9, 12, 13)
The WHO is the directing and coordinating authority – WHO controls allocation of health products (Treaty Art 9); WHO will compulsorily acquire 10% the health products each country produces – Art 12 (3); countries expected to set aside a portion of all the products they have - Treaty Art 13bis(2), and not stockpile - Treaty Art 13(4)
Increased role for WHO as global product-authorising agency; mutual recognition of regulatory approvals, for faster approval of health products (Treaty Art 14) (a varation of this has been included in the amendments to the IHR)
One Health – “balancing and “optimising” the health of people, planet, animals (Treaty Art 1)
Outlawing use of off-label drugs – limiting options - dictating clinical approach (Treaty Art 14) (a variation of this has been included in the amendments to the IHR - WHO can issue clinical guidance)
Always on – provisions apply “both during and between pandemics, unless otherwise specified” (Treaty Art 2); benefit sharing applies during any kind of PHEIC not just pandemics (Treaty Art 12(4); parties to collaborate “during and between pandemics” (Treaty Art 13(2))
Influencing public opinion - “promoting the use of social and behavioural sciences, risk communication and community engagement for pandemic prevention, preparedness and response” (Treaty Art 6(2)(d), 17, 18)
Establishing a global health emergency workforce to be deployable on request (Treaty Art 7)
Regulation of research and development (Treaty Art 9)
Global system for liability and compensation for vaccine injuries (Treaty Art 13(6)
Sovereignty is preserved – countries choose to enlist in the scheme, and countries do the implementation
New One Health treaty in the pipeline by 31 May 2026 (Treaty Art 5)
New bureaucracies - Global Supply Chain and Logistics Network (Treaty Art 13); Conference of the Parties (Treaty Art 21)
It doesn't mean much for Oklahoma : https://oklahomavoice.com/briefs/oklahoma-governor-signs-bill-exempting-state-from-who-and-un-mandates/#:~:text=OKLAHOMA%20CITY%20%E2%80%93%20Oklahoma%20will%20not,Gov.%20Kevin%20Stitt%20on%20Wednesday What is wrong with the insipid country of Australia?
The writing on the wall is there for all to see yet a toxic cohort of the population choose to be blind to anythng that challenged their perceived place in the herd. I would suggest that as many people of rational disposition get training in marshal arts and weapons training. Hanging on to the false belief that our governments are part of wholesome civil society when it is plain they are treasonous mercenaries of the genocidal Billionaire Eugenicists will only ensure a complete lack of preparedness for what is so blatantly a tyranny that has been more than a generation in the making.